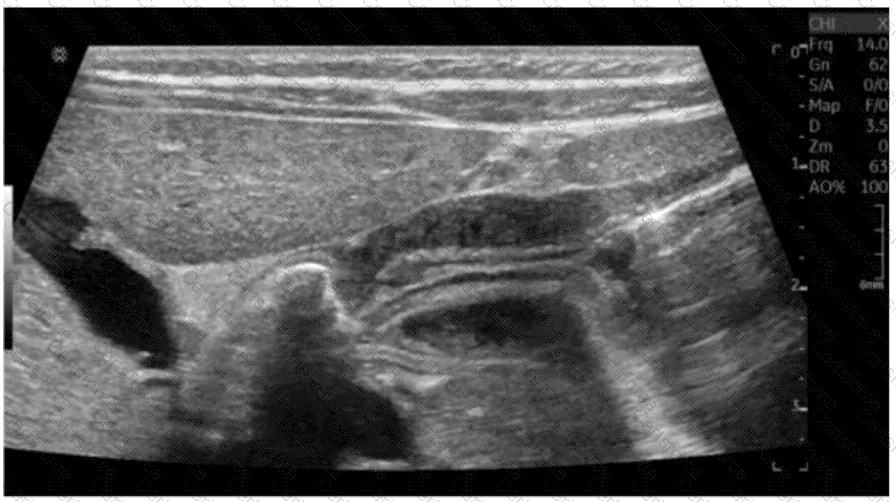
The ultrasound image shows a classic longitudinal view of a markedly thickened pyloric muscle with an elongated pyloric channel. This finding is consistent with hypertrophic pyloric stenosis (HPS), a condition most commonly seen in male infants between 2 and 8 weeks of age.
The most characteristic clinical finding associated with HPS is an “olive-shaped” palpable mass in the right upper quadrant or epigastric region, which represents the hypertrophied pylorus.
Clinical presentation of HPS includes:
Non-bilious projectile vomiting (due to gastric outlet obstruction)
Dehydration and weight loss
A palpable “olive” mass on physical exam
Visible peristalsis may be noted on the abdominal wall
Sonographic diagnostic criteria for HPS:
Pyloric muscle thickness ≥ 3 mm
Pyloric channel length ≥ 15–17 mm
“Cervix sign” or “target sign” (transverse view)
Failure of gastric contents to pass through the pylorus on real-time imaging
Differentiation from other options:
B. Fever of unknown origin: Not characteristic of HPS.
C. Red currant jelly stools: Classic for intussusception.
D. Bilious vomiting: Seen in distal duodenal or jejunal obstruction, not in pyloric stenosis (vomiting is non-bilious in HPS).
[References:, Rumack CM, Wilson SR, Charboneau JW, Levine D. Diagnostic Ultrasound. 5th Edition. Elsevier, 2018. Chapter: Gastrointestinal Tract, pp. 474–479., American College of Radiology (ACR). Appropriateness Criteria – Vomiting in Infants Up to 3 Months of Age., Radiopaedia.org. Hypertrophic pyloric stenosis:https://radiopaedia.org/articles/hypertrophic-pyloric-stenosis, ]
Submit