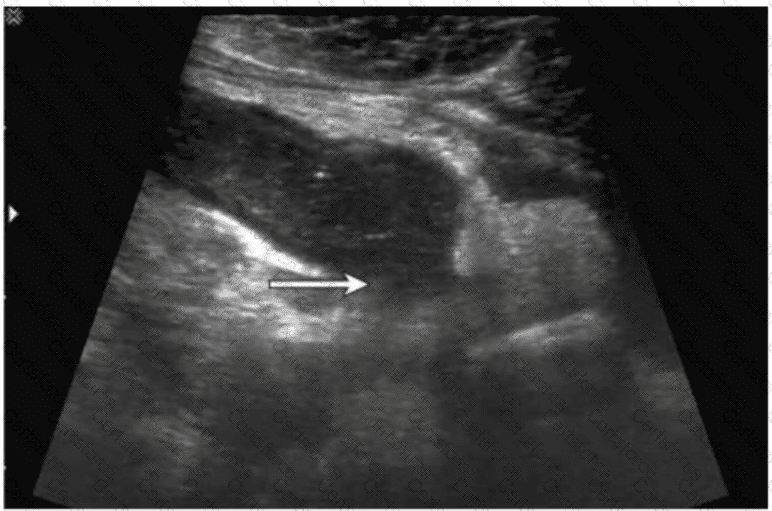
The ultrasound image demonstrates a tubular, non-compressible, blind-ending structure located in the right lower quadrant (RLQ) with associated echogenic periappendiceal fat and possibly adjacent fluid or phlegmon. These features are consistent with appendicitis. Given the clinical history of fever and RLQ pain, along with the irregular borders and complex periappendiceal findings, the diagnosis of a ruptured appendix is most likely.
Key sonographic features of ruptured appendicitis include:
Non-visualization or distortion of the normal appendiceal wall architecture
Periappendiceal fluid collection or abscess
Disruption of the echogenic submucosal layer
Surrounding fat stranding (hyperechoic inflammatory changes)
Clinical correlation with fever and peritonitis
Comparison of answer choices:
A. Bowel obstruction typically shows dilated bowel loops with air-fluid levels, not a tubular structure like the appendix.
B. Intussusception presents with a target or “donut” sign in a transverse view, not a linear tubular structure.
C. Enlarged lymph nodes are usually round or oval and hypoechoic with a central echogenic hilum, without a tubular appearance.
D. Ruptured appendix — Correct. The ultrasound features and clinical presentation match.
[References:, Rumack CM, Wilson SR, Charboneau JW, Levine D. Diagnostic Ultrasound, 5th ed. Elsevier; 2017., Jeffrey RB, Laing FC, Townsend RR. Acute appendicitis: sonographic criteria based on 250 cases. Radiology. 1988;167(2):327–329., American Institute of Ultrasound in Medicine (AIUM) Practice Parameter for the Performance of the Ultrasound Examination for Appendicitis (2020)., , ]
Submit